What is hysteroscopy?
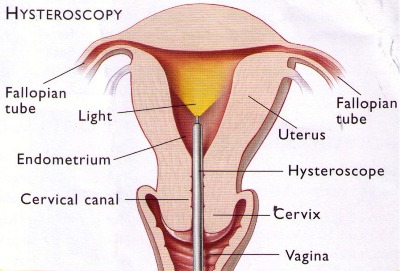
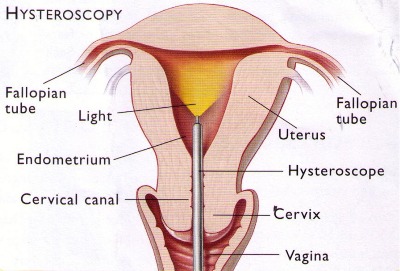
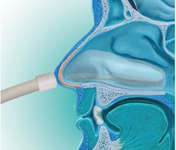
Hysteroscopy is a procedure that allows a doctor to look inside the uterus in order to diagnose and treat causes of abnormal bleeding. Hysteroscopy is done using a hysteroscope – a thin, lighted tube that is inserted into the vagina to examine the cervix and inside of the uterus.
Why is hysteroscopy done?
One of the most common uses for hysteroscopy is to find the cause of abnormal uterine bleeding. Abnormal bleeding can mean that a woman’s menstrual periods are heavier or longer than usual or occur less often or more often than normal. Bleeding between menstrual periods also is abnormal. Hysteroscopy may be either diagnostic or operative.
What is diagnostic hysteroscopy?
Diagnostic hysteroscopy is used to diagnose problems of the uterus such as abnormal uterine bleeding, infertility, repeated miscarriages, adhesions, fibroids, polyps, or to locate displaced intrauterine devices (IUDs). It may also be used to confirm the results of other tests such as hysterosalpingography (HSG). Other instruments or techniques, such as dilation and curettage (D&C) and laparoscopy, are sometimes used in conjunction with the hysteroscopy.
What is operative hysteroscopy?
Operative hysteroscopy is used to correct an abnormal condition that has been detected during a diagnostic hysteroscopy, avoiding the need for a second surgery. During operative hysteroscopy, small instruments used to correct the condition are inserted through the hysteroscope.
When is operative hysteroscopy used?
Hysteroscopy may be performed to correct the following uterine conditions:
- Polyps and fibroids – Hysteroscopy is used to remove these non-cancerous growths found in the uterus.
- Adhesions – also known as Asherman’s Syndrome, uterine adhesions are bands of scar tissue that can form in the uterus and may lead to changes in menstrual flow as well as infertility. Hysteroscopy can help locate and remove the adhesions.
- Septums – Hysteroscopy can help determine whether you have a uterine septum, a malformation of the uterus that is present from birth.
- Infertility – tubal blockage at uterine end can be opened through hysteroscopy by cornual cannulation
- Abnormal bleeding – Hysteroscopy can help identify the cause of heavy or lengthy menstrual flow, as well as bleeding between periods.
- Postmenopausal bleeding – Hysteroscopy is also performed to determine the cause of unexplained bleeding or spotting in postmenopausal women
- Removal of foreign body or a missing IUCD
What are the benefits of hysteroscopy?
Compared with other, more invasive procedures, hysteroscopy may provide the following advantages:
- Shorter hospital stay
- Shorter recovery time
- Less pain medication needed after surgery
- Avoidance of hysterectomy
- Possible avoidance of “open” abdominal surgery
How safe is hysteroscopy?
Hysteroscopy is a relatively safe procedure. However, as with any type of surgery, complications are possible. With hysteroscopy, complications occur in less than 1 percent of cases and can include:
- Risks associated with anesthesia
- Infection
- Heavy bleeding
- Injury to the cervix, uterus, adjacent organs
- Intrauterine scarring
When should the procedure be performed?
It may be recommended to schedule the hysteroscopy for the first week after your menstrual period. This timing will provide the doctor with the best view of the inside of the uterus.
What type of anesthesia is used for hysteroscopy?
Anesthesia for hysteroscopy may be local, regional, or general:
How is hysteroscopy performed?
Prior to the procedure, one may be prescribed a medication to help you relax. You will then be prepared for anesthesia. The hysteroscope is inserted through vagina and cervix into the uterus. Saline is then inserted into the uterus, through the hysteroscope, to expand it and to clear away any blood or mucus. A light shone through the hysteroscope allows the doctor to see inside the uterus and the openings of the fallopian tubes into the uterine cavity. Finally, if surgery needs to be performed, small instruments are inserted into the uterus through the hysteroscope.
The time it takes to perform hysteroscopy can range from less than 5 minutes to more than an hour. The length of the procedure depends on whether it is diagnostic or operative and whether an additional procedure, such as laparoscopy, is planned at the same time.
How will I be prepared for hysteroscopy?
If you are having general anesthesia in the hospital, you will be told not to eat or drink anything for a certain period of time (usually after midnight the night before) before the procedure. Routine lab tests may be ordered as well for women having a hysteroscopy in the hospital. You will be asked to empty your bladder and your vaginal area will be cleansed with an antiseptic
What can I expect after the procedure?
If regional or general anesthesia is used during your procedure, you may have to be observed for several hours before going home. After the procedure, you may have some cramping or slight vaginal bleeding for one to two days. However, if you experience any of the following symptoms, be sure to contact your doctor:
- Fever
- Severe abdominal pain
- Heavy vaginal bleeding or discharge
Will I have to stay in the hospital overnight?
Hysteroscopy is considered minor surgery and usually does not require an overnight stay in the hospital. However, in certain circumstances, such as if your doctor is concerned about your reaction to anesthesia an overnight stay may be required.
Who is a candidate for this procedure?
Although there are many benefits associated with hysteroscopy, it may not be appropriate for some patients. A doctor who specializes in this procedure will consult with your primary care physician to determine whether it is appropriate for you.














 Attention deficit / hyperactivity disorder (ADHD) is a highly prevalent condition in children that has generated considerable public interest and debate. It is a chronic, pervasive childhood disorder characterized by developmentally inappropriate activity level, low frustration tolerance, impulsivity, poor organization of behavior, distractibility, and inability to sustain attention and concentration (American Psychiatric Association, 2000)which occurs in 3% to 7% of school-age children (Egger et al., 2000).
Attention deficit / hyperactivity disorder (ADHD) is a highly prevalent condition in children that has generated considerable public interest and debate. It is a chronic, pervasive childhood disorder characterized by developmentally inappropriate activity level, low frustration tolerance, impulsivity, poor organization of behavior, distractibility, and inability to sustain attention and concentration (American Psychiatric Association, 2000)which occurs in 3% to 7% of school-age children (Egger et al., 2000). The right prefrontal cortex, vermis region of the cerebellum, caudate nucleus, and the globus pallidus are significantly smaller in children with ADHD than the normal children. Parents of children with ADHD are often noted to be experiencing mental difficulties, high levels of stress, and conflict- laden parent – child interactions. Non-genetic factors that are known to be linked to ADHD include premature birth, maternal alcohol and tobacco use, complications during pregnancy or birth and illnesses of early infancy, exposure to high levels of lead in early childhood, brain injuries that involve prefrontal cortex, overstimulation hypothesis, and metabolic dysfunction of the central nervous system.
The right prefrontal cortex, vermis region of the cerebellum, caudate nucleus, and the globus pallidus are significantly smaller in children with ADHD than the normal children. Parents of children with ADHD are often noted to be experiencing mental difficulties, high levels of stress, and conflict- laden parent – child interactions. Non-genetic factors that are known to be linked to ADHD include premature birth, maternal alcohol and tobacco use, complications during pregnancy or birth and illnesses of early infancy, exposure to high levels of lead in early childhood, brain injuries that involve prefrontal cortex, overstimulation hypothesis, and metabolic dysfunction of the central nervous system. Evidence based treatments for ADHD include behavioral interventions such as parent behavior management training, contingency management, and cognitive- behavior therapies, administered individually or in group settings, or pharmacologic treatment, with a variety of stimulant formulations and the non-stimulant atomoxetine approved for this indication. For many patients, the optimal treatment is multimodal, meaning the combination of medication and psychosocial treatments addressing all the impaired areas of life.
Evidence based treatments for ADHD include behavioral interventions such as parent behavior management training, contingency management, and cognitive- behavior therapies, administered individually or in group settings, or pharmacologic treatment, with a variety of stimulant formulations and the non-stimulant atomoxetine approved for this indication. For many patients, the optimal treatment is multimodal, meaning the combination of medication and psychosocial treatments addressing all the impaired areas of life.
 sees around him/her. Use rhymes such as jonny jonny yes papa. Encourage the child to say hahahahaa/aaaaaa with you. Associate the object with sound e,g introduce the clock to the child, t-t-t-t-t clock, ding- dong- ding-dong .pi pi pi pi daddy car. Make him listen to the sounds of objects and create a sound associated with the object. mow mow mow mow cow. Use the sound like p-p-p-p-, m-m-m-m-, b-b-b-b-b, brooo-brooo, grrrr- ggrr while bathing, playing with toys, pampering him/her. These sounds will help him to learn better in preschool and kindergarten. Expand on words what the child says, for an example, if (s)he says car or sound likes car. Expand on words saying oh! yes it is a CAR, Biiig CAR, Big red CAR! Show the child big colorful picture book with large pictures. Name them, read aloud and talk about the picture. Wait your child to explore the picture, Ask him/her what is this and you answer. Make him/her point to picture Repeat the same several days. You would be surprised one day hearing(s)he names the picture.
sees around him/her. Use rhymes such as jonny jonny yes papa. Encourage the child to say hahahahaa/aaaaaa with you. Associate the object with sound e,g introduce the clock to the child, t-t-t-t-t clock, ding- dong- ding-dong .pi pi pi pi daddy car. Make him listen to the sounds of objects and create a sound associated with the object. mow mow mow mow cow. Use the sound like p-p-p-p-, m-m-m-m-, b-b-b-b-b, brooo-brooo, grrrr- ggrr while bathing, playing with toys, pampering him/her. These sounds will help him to learn better in preschool and kindergarten. Expand on words what the child says, for an example, if (s)he says car or sound likes car. Expand on words saying oh! yes it is a CAR, Biiig CAR, Big red CAR! Show the child big colorful picture book with large pictures. Name them, read aloud and talk about the picture. Wait your child to explore the picture, Ask him/her what is this and you answer. Make him/her point to picture Repeat the same several days. You would be surprised one day hearing(s)he names the picture.
 Subsequently, this often results in chronic depression, poor scholastic performance, psycho-social problems, substance abuse and even suicide. It’s equally prevalent in both sexes during pre-puberty stage whereas more in females with a ratio of 2:1 post-puberty. Mean duration of an episode of depression is 7 to 9 months. 70 to 80 % recover at the end of one year. Increased chance of recurrence is seen in children with early onset and those with the history of previous episodes, co-morbid psychotic symptoms, poor drug compliance, negative life events and positive family history in parents. 20 to 30 % of depressive children develop manic episodes (Bipolar Disorder) on follow up.
Subsequently, this often results in chronic depression, poor scholastic performance, psycho-social problems, substance abuse and even suicide. It’s equally prevalent in both sexes during pre-puberty stage whereas more in females with a ratio of 2:1 post-puberty. Mean duration of an episode of depression is 7 to 9 months. 70 to 80 % recover at the end of one year. Increased chance of recurrence is seen in children with early onset and those with the history of previous episodes, co-morbid psychotic symptoms, poor drug compliance, negative life events and positive family history in parents. 20 to 30 % of depressive children develop manic episodes (Bipolar Disorder) on follow up. Few predisposing factors/ vulnerability factors are: Genetic; biological factors (neurotransmitters -monoamine metabolism and endocrine abnormalities); and temperament (e.g. quiet children with regular habits and slow to adapt to new experiences). Chronic life adversities are also likely to contribute to develop depression – broken homes, parental alcoholism, abuse, rejection etc. Undesirable life events in previous 12 months are important e.g., an event at home, or school and experience of loss.
Few predisposing factors/ vulnerability factors are: Genetic; biological factors (neurotransmitters -monoamine metabolism and endocrine abnormalities); and temperament (e.g. quiet children with regular habits and slow to adapt to new experiences). Chronic life adversities are also likely to contribute to develop depression – broken homes, parental alcoholism, abuse, rejection etc. Undesirable life events in previous 12 months are important e.g., an event at home, or school and experience of loss. disability by obtaining the history from all available sources; to explore into the stressors in the school/home; to consider differential diagnosis – Physical conditions like hypothyroidism; psychosis; normal reactive feelings of sadness and unhappiness; look for co morbid condition.
disability by obtaining the history from all available sources; to explore into the stressors in the school/home; to consider differential diagnosis – Physical conditions like hypothyroidism; psychosis; normal reactive feelings of sadness and unhappiness; look for co morbid condition.
 It is important for these people to see a Surgeon at the earliest to enable an accurate diagnosis and initiate early treatment to prevent further complications. Over the counter medications and creams are of limited use as almost all of these conditions present with more or less the same complaints, however the treatment is completely different for each one of them.
It is important for these people to see a Surgeon at the earliest to enable an accurate diagnosis and initiate early treatment to prevent further complications. Over the counter medications and creams are of limited use as almost all of these conditions present with more or less the same complaints, however the treatment is completely different for each one of them. These however, need to be performed by experienced Surgeons who have undergone extensive training in this specialty and have the know how and technical expertise.
These however, need to be performed by experienced Surgeons who have undergone extensive training in this specialty and have the know how and technical expertise.
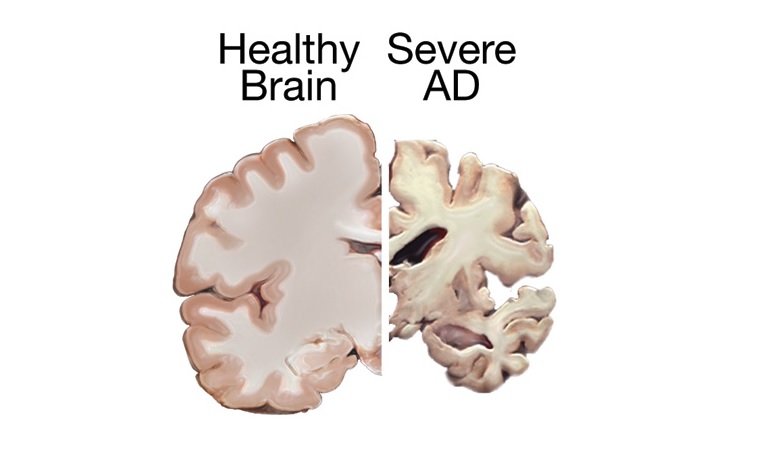
 Alzheimer’s disease is an irreversible, progressive brain disorder that slowly destroys memory and thinking skills, and eventually the ability to carry out the simplest tasks. Alzheimer’s is a type of dementia that causes problems with memory, thinking and behavior. Symptoms usually develop slowly and get worse over time, becoming severe enough to interfere with daily tasks.
Alzheimer’s disease is an irreversible, progressive brain disorder that slowly destroys memory and thinking skills, and eventually the ability to carry out the simplest tasks. Alzheimer’s is a type of dementia that causes problems with memory, thinking and behavior. Symptoms usually develop slowly and get worse over time, becoming severe enough to interfere with daily tasks. People with memory loss or other possible signs of Alzheimer’s may find it hard to recognize they have a problem. Signs of dementia may be more obvious to family members or friends. Anyone experiencing dementia-like symptoms should see a doctor as soon as possible. At International Modern Hospital, we offer specialised care for such patients under the guidance of our psychiatrist,
People with memory loss or other possible signs of Alzheimer’s may find it hard to recognize they have a problem. Signs of dementia may be more obvious to family members or friends. Anyone experiencing dementia-like symptoms should see a doctor as soon as possible. At International Modern Hospital, we offer specialised care for such patients under the guidance of our psychiatrist, 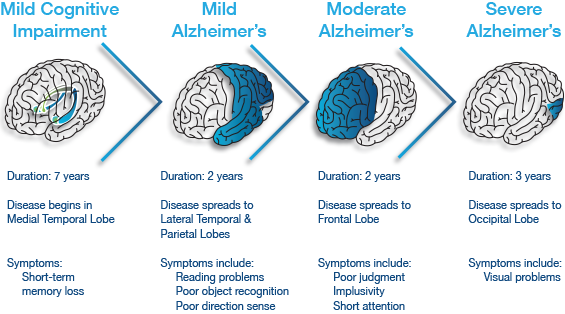
 Plaques are deposits of a protein fragment called beta-amyloid (BAY-tuh AM-uh-loyd) that build up in the spaces between nerve cells.
Plaques are deposits of a protein fragment called beta-amyloid (BAY-tuh AM-uh-loyd) that build up in the spaces between nerve cells.
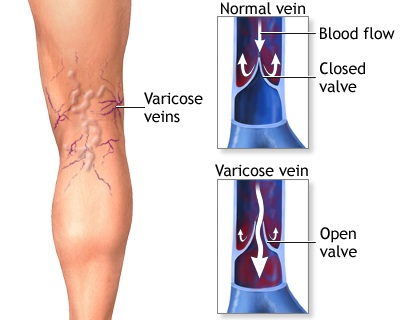
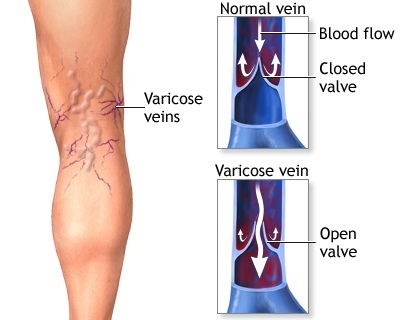 Varicose veins are swollen, twisted, and enlarged veins that you can see under the skin. They are often red or blue in color. They usually appear in the legs, but can occur in other parts of the body.
Varicose veins are swollen, twisted, and enlarged veins that you can see under the skin. They are often red or blue in color. They usually appear in the legs, but can occur in other parts of the body. Anorexia Nervosa is a psychological and possibly life-threatening eating disorder defined by an extremely low body weight relative to stature (this is called BMI [Body Mass Index] and is a function of an individual’s height and weight), extreme and needless weight loss, illogical fear of weight gain, and distorted perception of self-image and body.
Anorexia Nervosa is a psychological and possibly life-threatening eating disorder defined by an extremely low body weight relative to stature (this is called BMI [Body Mass Index] and is a function of an individual’s height and weight), extreme and needless weight loss, illogical fear of weight gain, and distorted perception of self-image and body.