“Depression – Let’s talk”, the World Health Day theme 2017 ring an alarm bell in our heart about the presence of this disorder amid our dear n’ near ones. Depression was once thought to be a disease of adults. It is no more considered rare among the children and adolescents, with an incidence of 2 – 4% and 4 – 8 % respectively. A youngster who appears withdrawn and lonely is most likely going through a period of “intense internal emotional turmoil”. They often feel sad and may consistently understand their plight as hopeless. They may frequently show poor concentration, lack of initiation; poor sleep and eating habits, negativity, get tired easily, feel guilty or worthless etc.  Subsequently, this often results in chronic depression, poor scholastic performance, psycho-social problems, substance abuse and even suicide. It’s equally prevalent in both sexes during pre-puberty stage whereas more in females with a ratio of 2:1 post-puberty. Mean duration of an episode of depression is 7 to 9 months. 70 to 80 % recover at the end of one year. Increased chance of recurrence is seen in children with early onset and those with the history of previous episodes, co-morbid psychotic symptoms, poor drug compliance, negative life events and positive family history in parents. 20 to 30 % of depressive children develop manic episodes (Bipolar Disorder) on follow up.
Subsequently, this often results in chronic depression, poor scholastic performance, psycho-social problems, substance abuse and even suicide. It’s equally prevalent in both sexes during pre-puberty stage whereas more in females with a ratio of 2:1 post-puberty. Mean duration of an episode of depression is 7 to 9 months. 70 to 80 % recover at the end of one year. Increased chance of recurrence is seen in children with early onset and those with the history of previous episodes, co-morbid psychotic symptoms, poor drug compliance, negative life events and positive family history in parents. 20 to 30 % of depressive children develop manic episodes (Bipolar Disorder) on follow up.
Majority of them may reach the general practitioner or the pediatrician with vague so called ‘functional symptoms’. A recent change in behavior with sad or irritable mood lasting for more than 2 weeks indicates a depression. Unfortunately, these disorders often go unrecognized by families and physicians alike. Early diagnosis and treatment of depressive disorders are critical to healthy emotional, social and behavioral development.
Clinical presentation varies according to the developmental stage of the child. They can be seen as given below:
Preschool child: apathetic, refuses food, unhappy and irritable, looks miserable, frequent crying spells, ‘failure to thrive’, insecure and unhappy child without any physical abnormality.
Middle childhood (Pre-adolescence): Apathy, verbal and motor retardation, and loss of appetite are the classic features of depression in this age group. Other features are: psychosomatic symptoms (e.g., head ache or pain abdomen); decline in academic performance with poor attention and concentration, irritability and social withdrawal, low self-esteem (I am not good enough compared to others), feeling bored and lack of interest in usual activities, sleep and appetite disturbances may be present though less common.
Adolescence: Clinical features are more similar to those of adult depression. Feeling sad, apathetic, lack of energy; sleep and appetite disturbances are more common. Bodily preoccupation, worries over his/her appearance or minor health problems (e.g., acne); suicidal thoughts are relatively common.
Etiology: There are multiple factors which individually or in combination with other factors, could contribute to depression.  Few predisposing factors/ vulnerability factors are: Genetic; biological factors (neurotransmitters -monoamine metabolism and endocrine abnormalities); and temperament (e.g. quiet children with regular habits and slow to adapt to new experiences). Chronic life adversities are also likely to contribute to develop depression – broken homes, parental alcoholism, abuse, rejection etc. Undesirable life events in previous 12 months are important e.g., an event at home, or school and experience of loss.
Few predisposing factors/ vulnerability factors are: Genetic; biological factors (neurotransmitters -monoamine metabolism and endocrine abnormalities); and temperament (e.g. quiet children with regular habits and slow to adapt to new experiences). Chronic life adversities are also likely to contribute to develop depression – broken homes, parental alcoholism, abuse, rejection etc. Undesirable life events in previous 12 months are important e.g., an event at home, or school and experience of loss.
Some points to be considered by a parent or caregivers to alleviate emotional disturbances:
- Use positive reinforcement while disciplining them; avoid overprotecting and over directing.
- Don’t expect absolute compliance. Don’t use your child to fulfill your own unachieved goals.
- Take the problem seriously. It will be important to them and give them a feel of being understood.
- Encourage them to talk to other people (may be a trusted adult friend or grandparents) as well as to you.
- Treatment strategies for Depression – right time; right way; right people
A proper assessment is needed to establish depression – understand the nature, extent and  disability by obtaining the history from all available sources; to explore into the stressors in the school/home; to consider differential diagnosis – Physical conditions like hypothyroidism; psychosis; normal reactive feelings of sadness and unhappiness; look for co morbid condition.
disability by obtaining the history from all available sources; to explore into the stressors in the school/home; to consider differential diagnosis – Physical conditions like hypothyroidism; psychosis; normal reactive feelings of sadness and unhappiness; look for co morbid condition.
Treatment can include a combination of pharmacological management and various psychotherapeutic approaches – Supportive counseling and ways to relieve stress; Cognitive behavior therapy; Interpersonal therapy.
To conclude, Depression is a treatable emotional/behavioral condition. What is needed is treatment by “right technique at right time by right people” (trained mental health professionals).

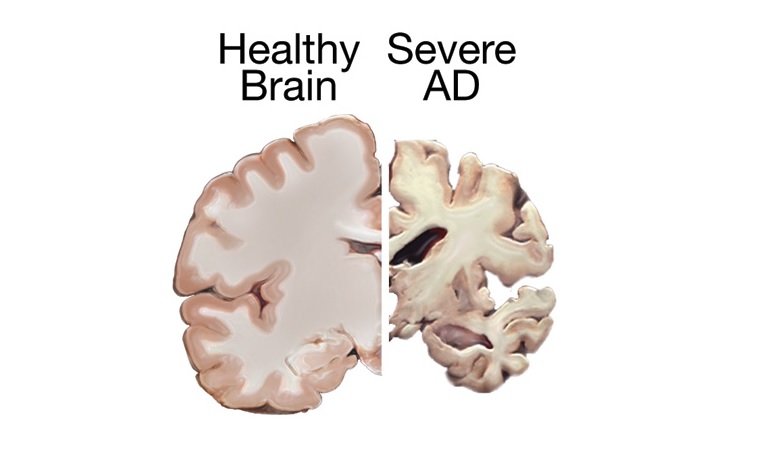
 Alzheimer’s disease is an irreversible, progressive brain disorder that slowly destroys memory and thinking skills, and eventually the ability to carry out the simplest tasks. Alzheimer’s is a type of dementia that causes problems with memory, thinking and behavior. Symptoms usually develop slowly and get worse over time, becoming severe enough to interfere with daily tasks.
Alzheimer’s disease is an irreversible, progressive brain disorder that slowly destroys memory and thinking skills, and eventually the ability to carry out the simplest tasks. Alzheimer’s is a type of dementia that causes problems with memory, thinking and behavior. Symptoms usually develop slowly and get worse over time, becoming severe enough to interfere with daily tasks. People with memory loss or other possible signs of Alzheimer’s may find it hard to recognize they have a problem. Signs of dementia may be more obvious to family members or friends. Anyone experiencing dementia-like symptoms should see a doctor as soon as possible. At International Modern Hospital, we offer specialised care for such patients under the guidance of our psychiatrist,
People with memory loss or other possible signs of Alzheimer’s may find it hard to recognize they have a problem. Signs of dementia may be more obvious to family members or friends. Anyone experiencing dementia-like symptoms should see a doctor as soon as possible. At International Modern Hospital, we offer specialised care for such patients under the guidance of our psychiatrist, 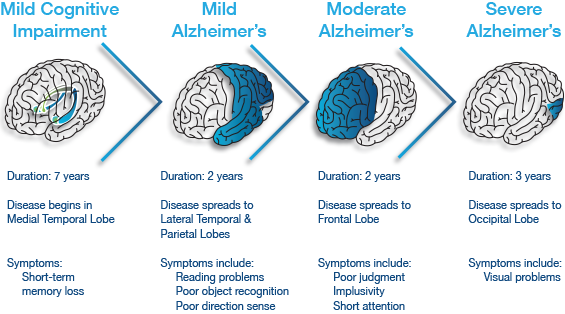
 Plaques are deposits of a protein fragment called beta-amyloid (BAY-tuh AM-uh-loyd) that build up in the spaces between nerve cells.
Plaques are deposits of a protein fragment called beta-amyloid (BAY-tuh AM-uh-loyd) that build up in the spaces between nerve cells.
 Anorexia Nervosa is a psychological and possibly life-threatening eating disorder defined by an extremely low body weight relative to stature (this is called BMI [Body Mass Index] and is a function of an individual’s height and weight), extreme and needless weight loss, illogical fear of weight gain, and distorted perception of self-image and body.
Anorexia Nervosa is a psychological and possibly life-threatening eating disorder defined by an extremely low body weight relative to stature (this is called BMI [Body Mass Index] and is a function of an individual’s height and weight), extreme and needless weight loss, illogical fear of weight gain, and distorted perception of self-image and body.